
What the most significant pharmacovigilance update in over a decade means for your team and for patients everywhere.
Imagine a world where a drug’s hidden risks are caught not by a flood of adverse event reports months after harm is done, but by an AI-powered system scanning real-world data in near real-time and flagging a pattern before it becomes a crisis. That world is no longer hypothetical. With the European Medicines Agency’s (EMA) sweeping Good Pharmacovigilance Practices (GVP) updates taking legal effect in February 2026, it is the new standard of care.
The 2026 GVP revision is not just a bureaucratic refresh. It represents a philosophical shift from a culture of passive documentation toward one of proactive, intelligent, patient-centered safety monitoring. Every pharmaceutical company operating in the European Union now has both a mandate and an opportunity to rethink how it approaches drug safety from the ground up.
EMA Pharmacovigilance Framework: From Volume 9A to the Age of AI
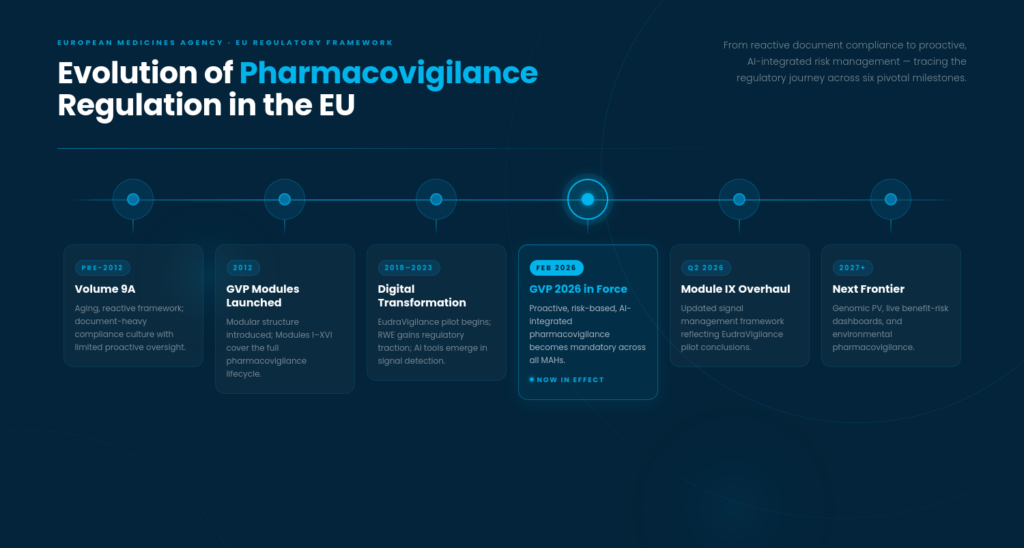
To appreciate just how far we have come, it helps to look back. Before 2012, EU pharmacovigilance was governed by the aging Volume 9A framework, a document-heavy, largely reactive system that struggled to keep pace with modern drug development. The landmark 2010 EU pharmacovigilance legislation triggered a complete rebuild, and by 2012, the GVP module system was born: a structured, modular framework covering everything from quality systems (Module I) to signal management (Module IX) to risk minimization (Module XVI).
For over a decade, those modules formed the backbone of drug safety compliance across Europe. Science moved on in the meantime. Real-world evidence emerged as a legitimate regulatory tool. Artificial intelligence crept into every corner of healthcare. EudraVigilance, the EU’s central safety database, grew into one of the world’s most powerful pharmacovigilance repositories. A global pandemic also reminded everyone that traditional safety timelines simply are not fast enough when lives are on the line.
The 2026 updates are the regulatory community’s answer to all of this.
5 Major EMA GVP 2026 Updates That Pharma Teams Need to Act On
1. Mothers, Babies, and a Long-Overdue Reckoning
For too long, pregnant and breastfeeding women occupied an uncomfortable gap in drug safety data. Clinical trials routinely exclude them, and post-market surveillance rarely followed the children born to mothers who took a medication during pregnancy. The result was a dangerous knowledge void that regulators, clinicians, and patients had to navigate without adequate evidence.
GVP Considerations P.III, which formally took effect on 9 February 2026, closes that gap with considerable precision. The guidance now mandates structured follow-up at birth, at three months, and at twelve months for children exposed either in utero or through breastmilk. It also clarifies that only maternal exposure to the product matters for reporting purposes, removing the confusion that plagued earlier iterations of the guideline.
This is about acknowledging that two patients are affected whenever a pregnant or breastfeeding woman takes a medicine. Pharmacovigilance teams will need to restructure their Individual Case Safety Report (ICSR) processes to capture these outcomes systematically, treating maternal and child follow-up as a core workflow rather than an edge case.
2. EudraVigilance Steps Into the Spotlight
Signal detection has long been a shared responsibility between regulators and industry, but the 2026 updates make one thing unmistakably clear: MAHs must now integrate EudraVigilance data directly into their own signal monitoring workflows. Following the formal conclusion of the EudraVigilance signal detection pilot, GVP Module IX on Signal Management is receiving a major overhaul expected in Q2 2026.
The new rules require Marketing Authorization Holders to screen EudraVigilance data at a frequency calibrated to each product’s specific safety profile. A product with a well-characterized risk profile may warrant monthly review, while a newer biological with emerging signals demands more frequent attention. The one-size-fits-all approach to signal detection cadence no longer applies.
MAHs are also no longer required to submit validated signals via standalone signal notification forms. Internal SOPs and processes now guide that workflow, with GVP Module IX as the governing reference. This demands a rigorous internal review of signal management procedures and clear role definitions across PV teams before the updated module takes effect.
3. AI and Digital Tools Move from Optional to Expected
Perhaps the most headline-grabbing change in the 2026 framework is this: the use of AI-powered pharmacovigilance tools is now expected, not optional. As the volume of global safety data continues to grow exponentially, manual processes simply cannot keep up. The EMA’s position is clear. Modern PV systems must leverage advanced analytics and automated signal detection to remain fit for purpose.
This aligns with the broader ICH M14 real-world evidence standard, which the EMA has embraced as a mechanism for post-market safety assessment. AI tools are no longer productivity enhancers sitting at the edge of the workflow; they are instruments of regulatory compliance sitting at its center.
For pharma teams, this creates immediate practical challenges. Which tools qualify under the framework? How do you validate an AI system for regulatory use? How do you maintain meaningful human oversight while still benefiting from automation? QA teams in particular will need to develop validation frameworks for AI systems and ensure audit trails that satisfy regulators during inspection.
4. Risk Minimization Measures Must Prove Their Worth
Designing a risk minimization measure, whether a Dear Healthcare Provider letter, a controlled access program, or a patient alert card, has always been a regulatory requirement. Under the 2026 framework, designing one is simply not enough. MAHs must now demonstrate that their RMMs actually reach the target population and influence clinical practice in a measurable way.
Periodic Safety Update Reports due for submission from February 2026 onward must include not just descriptions of RMMs, but concrete evidence of their effectiveness. Did the healthcare provider communication actually change prescribing behavior? Did the patient card reach the people who needed it most? Are the goals of risk minimization being achieved in everyday clinical settings?
For Regulatory Affairs teams, this means building effectiveness data collection into the post-approval plan from the start rather than searching for supporting evidence at PSUR submission time. It also means tighter alignment between the Risk Management Plan and real-world outcomes data, something that will require genuine cross-functional collaboration between PV, regulatory, and medical affairs.
5. Streamlined Operations with Firm New Boundaries
Not every update in the 2026 framework introduces a new compliance burden. The revised “Tell, Wait, and Do” procedure for low-risk variations genuinely streamlines the processing of minor changes to marketing authorizations, accelerating timelines and reducing administrative friction for routine updates that carry minimal safety implications.
The Pharmacovigilance System Master File also gets a welcome simplification. The new guidance focuses documentation requirements on major and critical deviations, freeing teams from the exhausting task of cataloguing every minor irregularity across a complex system. Directing PV resources toward material issues rather than administrative completeness is the underlying logic here.
One operational requirement, however, admits absolutely no flexibility. OMS (Organisation Management Service) registration is now a hard validation blocker, and submissions that include unregistered site information will be instantly rejected. For global companies with complex site structures, ensuring OMS/SPOR data accuracy across all entities sits at the top of the priority list.
What This Means Team by Team
PV and safety teams should focus on integration as the organizing principle: EudraVigilance into signal workflows, AI tools into case processing, and child health outcomes into pregnancy reporting. SOPs need updating, training needs refreshing, and the team needs to be comfortable with real-world evidence methodology before the next PSUR window opens.
Regulatory affairs teams face a closer eye on OMS/SPOR accuracy, a rethinking of how RMPs are structured around measurable risk outcomes, and adoption of electronic product information (ePI) formats where applicable. PSURs are no longer primarily safety narratives. They are evidence packages, and they will be evaluated as such.
QA and audit teams carry the responsibility of making the invisible visible: validating AI tools, auditing EudraVigilance screening processes, verifying maternal-child follow-up compliance, and ensuring that PSMF documentation is both lean and inspection-ready without sacrificing completeness on the issues that matter.
Looking Further Ahead
If the 2026 updates feel transformative, the trends shaping the next generation of pharmacovigilance look even more remarkable. Hyper-personalized drug safety monitoring, using genetic and genomic profiles to stratify risk at the individual patient level, is moving steadily from research concept toward regulatory consideration. Environmental pharmacovigilance, which examines the ecological impact of medicines excreted into water systems and soil, is gaining traction as a new area of MAH responsibility in several jurisdictions.
Patient-reported outcomes flowing directly into EudraVigilance could soon enable a form of crowd-sourced safety surveillance at a scale regulators could only imagine a decade ago. The static PSUR, a periodic snapshot of safety data frozen at a point in time, may ultimately give way to live benefit-risk dashboards offering continuous, rolling monitoring as digital infrastructure matures.
The trajectory is clear: drug safety is becoming faster, more inclusive, and more evidence-based with every regulatory cycle.
Conclusion
The EMA’s 2026 GVP updates are not a compliance hurdle to clear and forget. They are a directional signal about where pharmaceutical safety is heading and what companies must build today to remain fit for purpose tomorrow. Organizations that invest in the right systems, the right training, and the right data infrastructure will not simply be compliant; they will be genuinely better equipped to protect the patients who depend on the medicines they make.
That includes the pregnant patients, the nursing patients, and the patients whose adverse events were never quite visible in a clinical trial setting. Good pharmacovigilance has always been about finding them. The 2026 framework makes that obligation clearer than ever.
Why Choose DDReg for GVP 2026 Pharmacovigilance Compliance?
As the 2026 GVP framework raises the bar on signal detection, AI integration, and risk minimization evidence, having the right pharmacovigilance partner matters more than ever. DDReg brings together a global team of PV specialists, regulatory experts, and technology-driven workflows to support MAHs at every stage of the safety data lifecycle. From ICSR processing and EudraVigilance signal monitoring to PSUR preparation and RMP effectiveness assessment, DDReg delivers audit-ready, fully compliant pharmacovigilance services aligned with current EMA, ICH, and GVP standards. Companies navigating the 2026 transition rely on DDReg to move faster, reduce compliance risk, and keep patient safety at the center of every decision.
Stay ahead of EMA GVP compliance requirements and regulatory changes. Subscribe for expert updates from our pharmacovigilance team.